DIAGNOSIS OF BRAIN TUMOR

Google images
Although there is no specific or singular clinical symptom or sign for any brain tumors, the presence of a combination of symptoms and the lack of corresponding clinical indications of infections or other causes can be an indicator to redirect diagnostic investigation towards the possibility of an intracranial neoplasm. Brain tumors have similar characteristics and obstacles when it comes to diagnosis and therapy with tumors located elsewhere in the body. However, create specific issues that follow closely to the properties of the organ they are in.[10]
The diagnosis will often start with an interrogation of the patient to get a clear view of his medical antecedents, and his current symptoms. Clinical and laboratory investigations will serve to exclude infections as the cause of the symptoms. Examinations in this stage may include the eyes, otolaryngological (or ENT) and/or electrophysiological exams. The use of electroencephalography (EEG) often plays a role in the diagnosis of brain tumors.
Swelling, or obstruction of the passage of cerebrospinal fluid (CSF) from the brain may cause (early) signs of increased intracranial pressure which translates clinically into headaches, vomiting, or an altered state of consciousness, and in children changes to the diameter of the skull and bulging of the fontanelles. More complex symptoms such as endocrine dysfunctions should alarm doctors not to exclude brain tumors.
A bilateral temporal visual field defect (due to compression of the optic chiasm) or dilatation of the pupil, and the occurrence of either slowly evolving or the sudden onset of focal neurologic symptoms, such as cognitive and behavioral impairment (including impaired judgment, memory loss, lack of recognition, spatial orientation disorders), personality or emotional changes, hemiparesis, hypoesthesia,aphasia, ataxia, visual field impairment, impaired sense of smell, impaired hearing, facial paralysis, double vision, or more severe symptoms such as tremors, paralysis on one side of the body hemiplegia, or (epileptic) seizures in a patient with a negative history for epilepsy, should raise the possibility of a brain tumor.[10]
Imaging
Imaging plays a central role in the diagnosis of brain tumors. Early imaging methods—invasive and sometimes dangerous— such as pneumoencephalography and cerebralangiography, have been abandoned in recent times in favor of non-invasive, high-resolution techniques, especially magnetic resonance imaging (MRI) and computed tomography(CT)-scans. Neoplasms will often show as differently colored masses (also referred to as processes) in CT or MRI results.
The template Citation needed span is being considered for possible deletion.› Glioblastoma multiforme and anaplastic astrocytoma have been associated with the genetic acute hepaticporphyrias (PCT, AIP, HCP and VP), including positive testing associated with drug refractory seizures.[citation needed] Unexplained complications associated with drug treatments with these tumors should alert physicians to an undiagnosed neurological porphyria.
The definitive diagnosis of brain tumor can only be confirmed by histological examination of tumor tissue samples obtained either by means of brain biopsy or open surgery. The histological examination is essential for determining the appropriate treatment and the correct prognosis. This examination, performed by a pathologist, typically has three stages: interoperative examination of fresh tissue, preliminary microscopic examination of prepared tissues, and follow-up examination of prepared tissues after immunohistochemical staining or genetic analysis.[11]
Tests for brain tumours
MRI is a scan using magnetism. It usually gives the clearest picture of the brain of any type of scan and will almost certainly show up a brain tumour. You usually have an injection of contrast medium (see above) to make the MRI scan clearer.
It is very important to tell your doctor if you have any metal inside your body as this may mean you cannot have an MRI scan.[12]
You may have X-rays to check your general state of health. This will be important if you are diagnosed with a brain tumour because you may need to have surgery or intensive radiotherapy treatment.[12]
You may have blood tests to check for specific chemical markers in the blood. Some tumours, such as pineal region tumours or germ cell tumours may change the level of particular hormones and your doctor will check for these.[12]
Why you need more tests
These tests help the doctor to find out exactly what type of brain tumour you have. They also help the doctors to find out how big the tumour is. This information is important for the doctors to know which is the best treatment.
MRI is a scan using magnetism. MRI usually gives the clearest scan of the brain and spine and will almost certainly show up a brain tumour. You will usually have an injection of a dye, called contrast medium, to make the MRI scan clearer. Specialised MRI scans called Magnetic Resonance Angiography scans or MRA can show the blood vessels. Magnetic Resonance Spectroscopy or MRS look at chemicals in the tumour. You may need to have more than one MRI as your specialist gathers information about your condition.[13]
Taking a sample of tissue is the only sure way to diagnose many brain tumours. Looking at the cells under a microscope is the only guaranteed way to identify the type of brain tumour and grade of the tumour. For some brain tumours, you will have a biopsy as the first part of an operation to remove all or part of your tumour. For others, you may just have a biopsy and then go onto have other treatment such as radiotherapy. In some cases it is not possible to have a biopsy as the tumour is in an area of the brain that is too difficult to operate on. This may be because the tumour is close to major blood vessels or is in an area of the brain that controls vital functions in the body.
There is detailed information about having a biopsy in the section about surgery for brain tumours.
Lumbar puncture
A lumbar puncture is only used for certain types of brain tumour that can spread within the central nervous system. The test involves getting a sample of cerebrospinal fluid and examining it for cancer cells. Doctors can't always do this test on people with brain tumours. Sometimes, the pressure inside the brain and spinal canal (the intracranial pressure) is too high and to do a lumbar puncture would be dangerous. There is detailed information on having a lumbar puncture in the section about cancer tests.
Children usually have a sedative or a short general anaesthetic to have this test. There are two main reasons for this. It is very important to keep very still and they may find the test upsetting.[13]
Your doctor may ask you to have a scan of your tummy (abdomen) and a chest X-ray. The scan and X-ray are to check whether you have cancer anywhere else in your body. In adults, cancer that has spread to the brain (secondary brain tumour) is much more common than cancer that started in the brain (primary brain tumour). So it is sensible for your doctor to check. Ultrasound uses sound waves to build up a picture of the area being scanned. It is completely painless and only takes a few minutes.[13]
An angiogram examines the blood supply to the area being scanned. Angiograms are not done very often for brain tumours these days. But they are an important test for meningiomas and some othertypes of brain tumour. They give surgeons the following information.
For this test you usually have to go into hospital overnight. You will need a sedative or a general anaesthetic. You have the angiogram in the X-ray department. First, you have a tube (catheter) put into a blood vessel in your groin. The doctor injects a dye that shows up on X-ray into the tube. After a minute or so, the dye will have circulated through your bloodstream into the blood vessels into your brain. Your surgeon will look at your brain on an X-ray screen to see exactly how near the tumour is to the blood vessels.
Depending on the type of brain tumour you have, your surgeon may then inject something to block the blood vessels that carry blood to the tumour. This will help to shrink the tumour before you have surgery to remove it. This procedure is called embolisation or interventional angiography. There is a small risk of a stroke from this procedure. But the risk is usually small compared to the benefit of treating the tumour. Before you have this treatment, your specialist will explain all this to you and you will be able to ask questions or talk through any worries that you have.[13]
PET scans are a fairly new type of scan. They are not available at all hospitals. So if your specialist wants you to have one, you may have to travel to another hospital. PET scans can show up the rate of activity of body tissues. The scan traces a small amount of radioactive glucose that you have as an injection. The brain uses up the glucose and the scan measures how quickly this happens. The speed of glucose use by the area of the brain being scanned helps to show if a brain tumour is benign or malignant.[13]
SPECT stands for Single Photon Emission Computed Tomography. It is similar to a PET scan, but uses much simpler equipment to get information about chemicals in the brain tumour. As with a PET scan, you have an injection of a very small amount of a radioactive chemical. This does not harm you. The radioactive chemical circulates in your blood to your brain and shows up the brain tumour on the scanner.[13]
A myelogram gives pictures of the spinal cord. First you have a lumbar puncture. Then the doctor injects a dye into the area around the spinal cord. This is the space that the cerebrospinal fluid flows through. The dye spreads through this fluid. Then you have X-rays taken. If a tumour is blocking the flow of the fluid, the dye cannot get past it. And so the position of the tumour will show up on the X-rays.[13]
This test is done under general anaesthetic. A 2cm hole is drilled into the skull. A fine tube called a neuroendoscope is put into the hole and into the fluid filled chambers of the brain (the ventricles). This test may be done to[13]
What happens after the tests
You will be asked to go back to the hospital when your test results have come through. This is bound to take a little time, even if only a few days. You are likely to feel anxious during this time. While you are waiting for results it may help to talk to a close friend or relative about how you feel. Or you may want to contact a cancer support group to talk to someone who has been through a similar experience. If you want to find people to share experiences with online, you could use Cancer Chat, our online forum. Look in our general cancer organisations section for information about people who can offer support. Our counselling section has details of counselling organisations who can help you to find a counsellor in your area.[13]
The diagnosis will often start with an interrogation of the patient to get a clear view of his medical antecedents, and his current symptoms. Clinical and laboratory investigations will serve to exclude infections as the cause of the symptoms. Examinations in this stage may include the eyes, otolaryngological (or ENT) and/or electrophysiological exams. The use of electroencephalography (EEG) often plays a role in the diagnosis of brain tumors.
Swelling, or obstruction of the passage of cerebrospinal fluid (CSF) from the brain may cause (early) signs of increased intracranial pressure which translates clinically into headaches, vomiting, or an altered state of consciousness, and in children changes to the diameter of the skull and bulging of the fontanelles. More complex symptoms such as endocrine dysfunctions should alarm doctors not to exclude brain tumors.
A bilateral temporal visual field defect (due to compression of the optic chiasm) or dilatation of the pupil, and the occurrence of either slowly evolving or the sudden onset of focal neurologic symptoms, such as cognitive and behavioral impairment (including impaired judgment, memory loss, lack of recognition, spatial orientation disorders), personality or emotional changes, hemiparesis, hypoesthesia,aphasia, ataxia, visual field impairment, impaired sense of smell, impaired hearing, facial paralysis, double vision, or more severe symptoms such as tremors, paralysis on one side of the body hemiplegia, or (epileptic) seizures in a patient with a negative history for epilepsy, should raise the possibility of a brain tumor.[10]
Imaging
Imaging plays a central role in the diagnosis of brain tumors. Early imaging methods—invasive and sometimes dangerous— such as pneumoencephalography and cerebralangiography, have been abandoned in recent times in favor of non-invasive, high-resolution techniques, especially magnetic resonance imaging (MRI) and computed tomography(CT)-scans. Neoplasms will often show as differently colored masses (also referred to as processes) in CT or MRI results.
- Benign brain tumors often show up as hypodense (darker than brain tissue) mass lesions on cranial CT-scans. On MRI, they appear either hypo- (darker than brain tissue) or isointense (same intensity as brain tissue) on T1-weighted scans, or hyperintense (brighter than brain tissue) on T2-weighted MRI, although the appearance is variable.
- Contrast agent uptake, sometimes in characteristic patterns, can be demonstrated on either CT or MRI-scans in most malignant primary and metastatic brain tumors.
- Perifocal edema, or pressure-areas, or where the brain tissue has been compressed by an invasive process also appears hyperintense on T2-weighted MRI, they might indicate the presence a diffuse neoplasm (unclear outline)
The template Citation needed span is being considered for possible deletion.› Glioblastoma multiforme and anaplastic astrocytoma have been associated with the genetic acute hepaticporphyrias (PCT, AIP, HCP and VP), including positive testing associated with drug refractory seizures.[citation needed] Unexplained complications associated with drug treatments with these tumors should alert physicians to an undiagnosed neurological porphyria.
The definitive diagnosis of brain tumor can only be confirmed by histological examination of tumor tissue samples obtained either by means of brain biopsy or open surgery. The histological examination is essential for determining the appropriate treatment and the correct prognosis. This examination, performed by a pathologist, typically has three stages: interoperative examination of fresh tissue, preliminary microscopic examination of prepared tissues, and follow-up examination of prepared tissues after immunohistochemical staining or genetic analysis.[11]
Tests for brain tumours
- CT scan
MRI is a scan using magnetism. It usually gives the clearest picture of the brain of any type of scan and will almost certainly show up a brain tumour. You usually have an injection of contrast medium (see above) to make the MRI scan clearer.
It is very important to tell your doctor if you have any metal inside your body as this may mean you cannot have an MRI scan.[12]
You may have X-rays to check your general state of health. This will be important if you are diagnosed with a brain tumour because you may need to have surgery or intensive radiotherapy treatment.[12]
You may have blood tests to check for specific chemical markers in the blood. Some tumours, such as pineal region tumours or germ cell tumours may change the level of particular hormones and your doctor will check for these.[12]
Why you need more tests
These tests help the doctor to find out exactly what type of brain tumour you have. They also help the doctors to find out how big the tumour is. This information is important for the doctors to know which is the best treatment.
MRI is a scan using magnetism. MRI usually gives the clearest scan of the brain and spine and will almost certainly show up a brain tumour. You will usually have an injection of a dye, called contrast medium, to make the MRI scan clearer. Specialised MRI scans called Magnetic Resonance Angiography scans or MRA can show the blood vessels. Magnetic Resonance Spectroscopy or MRS look at chemicals in the tumour. You may need to have more than one MRI as your specialist gathers information about your condition.[13]
Taking a sample of tissue is the only sure way to diagnose many brain tumours. Looking at the cells under a microscope is the only guaranteed way to identify the type of brain tumour and grade of the tumour. For some brain tumours, you will have a biopsy as the first part of an operation to remove all or part of your tumour. For others, you may just have a biopsy and then go onto have other treatment such as radiotherapy. In some cases it is not possible to have a biopsy as the tumour is in an area of the brain that is too difficult to operate on. This may be because the tumour is close to major blood vessels or is in an area of the brain that controls vital functions in the body.
There is detailed information about having a biopsy in the section about surgery for brain tumours.
Lumbar puncture
A lumbar puncture is only used for certain types of brain tumour that can spread within the central nervous system. The test involves getting a sample of cerebrospinal fluid and examining it for cancer cells. Doctors can't always do this test on people with brain tumours. Sometimes, the pressure inside the brain and spinal canal (the intracranial pressure) is too high and to do a lumbar puncture would be dangerous. There is detailed information on having a lumbar puncture in the section about cancer tests.
Children usually have a sedative or a short general anaesthetic to have this test. There are two main reasons for this. It is very important to keep very still and they may find the test upsetting.[13]
Your doctor may ask you to have a scan of your tummy (abdomen) and a chest X-ray. The scan and X-ray are to check whether you have cancer anywhere else in your body. In adults, cancer that has spread to the brain (secondary brain tumour) is much more common than cancer that started in the brain (primary brain tumour). So it is sensible for your doctor to check. Ultrasound uses sound waves to build up a picture of the area being scanned. It is completely painless and only takes a few minutes.[13]
An angiogram examines the blood supply to the area being scanned. Angiograms are not done very often for brain tumours these days. But they are an important test for meningiomas and some othertypes of brain tumour. They give surgeons the following information.
- Which blood vessels are supplying the tumour
- If the tumour is attached to any major blood vessels in the brain
For this test you usually have to go into hospital overnight. You will need a sedative or a general anaesthetic. You have the angiogram in the X-ray department. First, you have a tube (catheter) put into a blood vessel in your groin. The doctor injects a dye that shows up on X-ray into the tube. After a minute or so, the dye will have circulated through your bloodstream into the blood vessels into your brain. Your surgeon will look at your brain on an X-ray screen to see exactly how near the tumour is to the blood vessels.
Depending on the type of brain tumour you have, your surgeon may then inject something to block the blood vessels that carry blood to the tumour. This will help to shrink the tumour before you have surgery to remove it. This procedure is called embolisation or interventional angiography. There is a small risk of a stroke from this procedure. But the risk is usually small compared to the benefit of treating the tumour. Before you have this treatment, your specialist will explain all this to you and you will be able to ask questions or talk through any worries that you have.[13]
PET scans are a fairly new type of scan. They are not available at all hospitals. So if your specialist wants you to have one, you may have to travel to another hospital. PET scans can show up the rate of activity of body tissues. The scan traces a small amount of radioactive glucose that you have as an injection. The brain uses up the glucose and the scan measures how quickly this happens. The speed of glucose use by the area of the brain being scanned helps to show if a brain tumour is benign or malignant.[13]
SPECT stands for Single Photon Emission Computed Tomography. It is similar to a PET scan, but uses much simpler equipment to get information about chemicals in the brain tumour. As with a PET scan, you have an injection of a very small amount of a radioactive chemical. This does not harm you. The radioactive chemical circulates in your blood to your brain and shows up the brain tumour on the scanner.[13]
- Myelogram
A myelogram gives pictures of the spinal cord. First you have a lumbar puncture. Then the doctor injects a dye into the area around the spinal cord. This is the space that the cerebrospinal fluid flows through. The dye spreads through this fluid. Then you have X-rays taken. If a tumour is blocking the flow of the fluid, the dye cannot get past it. And so the position of the tumour will show up on the X-rays.[13]
This test is done under general anaesthetic. A 2cm hole is drilled into the skull. A fine tube called a neuroendoscope is put into the hole and into the fluid filled chambers of the brain (the ventricles). This test may be done to[13]
- Take a biopsy of a tumour that is in or near the ventricles
- Take fluid samples for tests
- Drain fluid if too much has built up and caused an increase in pressure (hydrocephalus)
What happens after the tests
You will be asked to go back to the hospital when your test results have come through. This is bound to take a little time, even if only a few days. You are likely to feel anxious during this time. While you are waiting for results it may help to talk to a close friend or relative about how you feel. Or you may want to contact a cancer support group to talk to someone who has been through a similar experience. If you want to find people to share experiences with online, you could use Cancer Chat, our online forum. Look in our general cancer organisations section for information about people who can offer support. Our counselling section has details of counselling organisations who can help you to find a counsellor in your area.[13]
PATHOLOGY
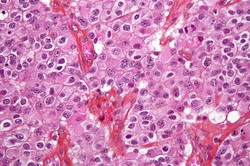
Google image
Micrograph of an oligodendroglioma, a type of brain cancer. Brain biopsy. H&E stain.
Tumors have characteristics that allow determination of its malignacy, how it will evolve and it will allow the medical team to determine the management plan.
- Anaplasia: or dedifferentiation; loss of differentiation of cells and of their orientation to one another and blood vessels, a characteristic of anaplastic tumor tissue. Anaplastic cells have lost total control of their normal functions and many have deteriorated cell structures. Anaplastic cells often have abnormally high nuclear-to-cytoplasmic ratios, and many are multinucleated. Additionally, the nuclei of anaplastic cells are usually unnaturally shaped or oversized nuclei. Cells can become anaplastic in two ways: neoplastic tumor cells can dedifferentiate to become anaplasias (the dedifferentiation causes the cells to lose all of their normal structure/function), or cancer stem cells can increase in their capacity to multiply (i.e., uncontrollable growth due to failure of differentiation).[14]
- Atypia: is an indication of abnormality of a cell (which may be indicative for malignancy). Significance of the abnormality is highly dependent on context.
- Neoplasia: is the (uncontrolled) division of cells; as such neoplasia is not problematic but its consequences are: the uncontrolled division of cells means that the mass of a neoplasm increases in size, and in a confined space such as the intracranial cavity this quickly becomes problematic because the mass invades the space of the brain pushing it aside, leading to compression of the brain tissue and increased intracranial pressure and destruction of brain parenchyma. Increased Intracranial pressure (ICP) may be attributable to the direct mass effect of the tumor, increased blood volume, or increased cerebrospinal fluid (CSF) volume may in turn have secondary symptoms
- Necrosis: is the (premature) death of cells, caused by external factors such as infection, toxin or trauma. Necrotic cells send the wrong chemical signals which preventsphagocytes from disposing of the dead cells, leading to a build up of dead tissue, cell debris and toxins at or near the site of the necrotic cells
Arterial and venous hypoxia, or the deprivation of adequate oxygen supply to certain areas of the brain, occurs when a tumor makes use of nearby blood vessels for its supply of blood and the neoplasm enters into competition for nutrients with the surrounding brain tissue.
More generally a neoplasm may cause release of metabolic end products (e.g., free radicals, altered electrolytes, neurotransmitters), and release and recruitment of cellular mediators (e.g., cytokines) that disrupt normal parenchymal function[14]
